kiny
Well-known member


Last edited:
If cipro is effective why is it not curative?
AIEC simply gains resistance to the antibiotic.
Cipro is able to get people into remission, but they don't stay in remission. When cipro is tried again, it generally fails due to the development of resistance due to prior exposure of cipro.
It's the same reason why urinary tract infections involving E Coli respond less and less to antibiotics, due to overuse of antibiotics, they simply developed resistance to the antibiotic.
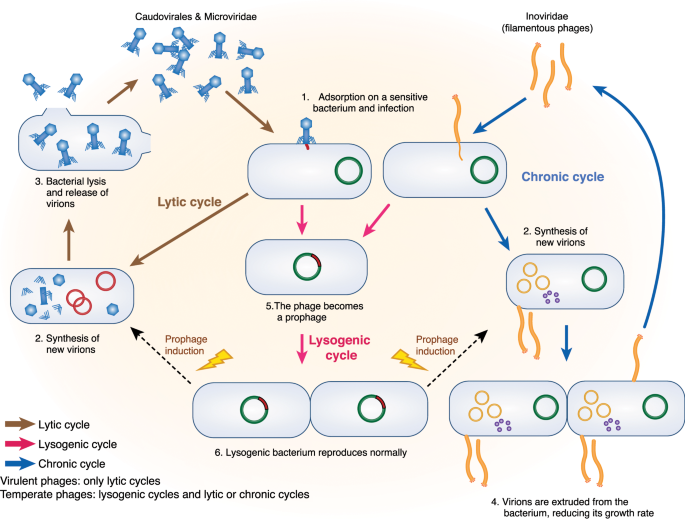
That's why phage therapy is in development for both crohn's disease and urinary tract infections, to overcome E Coli resistance.
Autoimmunity requires the identification of an adaptive response towards a self-antigen. This has never been identified in crohn's disease patients. Nor does it make any sense, mutations in ATG16L1, specific to crohn's disease and related to bacterial clearance (xenophagy), has no overlap whatsoever with autoimmune diseases. Autoimmunity in crohn's disease is a dead theory.Or it is an autoimmune disease and has nothing to do with E coli.
The duodenum lacks peyer's patches but there are in the mouth?The highest concentration of bacterial mass in the human body is in
-the ileum
-the colon
-the mouth
Crohn's disease manifests itself in
-the ileum
-the colon
-the mouth
Genetic mutations in NOD2, ATG16L1, strongly linked to crohn's disease, relate to bacterial recognition and bacterial clearance.
We use tests like anti-OmpC (antibodies to outer membrane E Coli) to diagnose crohn's disease.
We can now predict who will develop crohn's disease by looking at pathogenic bacterial populations in the intestine.
We can identify pathogenic species, a macrophage response, and T cell response, when we take biopsies from granuloma.
Bodies at the forefront of bacteriology, like Institut Pasteur, are involved in crohn's disease research.
I am pretty open minded regarding more obscure crohn's disease theories. The cold chain hypothesis, hygiene hypothesis.
But autoimmune theories that can't identify a self antigen, and ignore the bacterial link, are crackpot/conspiracy theories at this point.
The evidence linking bacteria to crohn's disease is beyond overwhelming at this point, it is undeniable.
There is a small amount of research suggesting that the intestinal permeability in crohn's disease is a result of a tight junction disorder in crohn's disease patients, which allows bacteria to enter tissue.My current hypothesis is that in most cases the bacteria are able to infiltrate in Crohn’s patients because of some kind of tissue damage in the gut, which itself could be due to a number of factors including impaired flow through a region of intestine, foods that cause chemical damage to the intestine, trauma, or acute infection.
 www.medpagetoday.com
www.medpagetoday.com

 www.everydayhealth.com
www.everydayhealth.com
Takeda Pharmaceutical has agreed to license, co-develop, and co-promote Enterome’s lead candidate, the Phase Ib Crohn’s disease candidate EB8018, Enterome said today, through a collaboration that could generate more than $690 million for the French biotech focused on treating microbiome-associated diseases.
EB8018 is a novel, first-in-class, oral gut-restricted small molecule designed to selectively disarm virulent bacteria in the gut that can cause inflammation without disrupting the local microbiome. Enterome has been developing EB8018 since licensing the small molecule for an undisclosed amount from its discoverer Vertex Therapeutics in 2016.
EB8018 is designed to work by inhibiting FimH-mediated inflammation induced by the interaction of pathogenic pro-inflammatory bacteria to receptors in the gut wall, thereby potentially reducing the production of inflammatory cytokines including TNF.
Together with Takeda, Enterome plans to launch a Phase II clinical proof-of-concept trial of EB8018 in 2019. The companies are also partnering on a Phase Ib trial (NCT03709628) that has begun recruiting patients, according to an update posted Friday on ClinicalTrials.gov.
The Phase Ib trial will consist of eight patients and two parts: Part 1 is designed to demonstrate that a single oral dose of EB8018 that is safe and tolerable in patients with Crohn’s disease, while Part 2 will characterize the PK profile when administered as multiple oral doses. The new trial is intended to support the development of EB8018 as an add-on therapy, for the treatment of adult patients suffering from Crohn’s disease.
Enterome said its agreement with Takeda covers the development of EB8018 in Crohn’s disease, with the potential to expand to other unspecified gastrointestinal (GI) disorders and liver diseases.
“We are delighted to sign this agreement for EB8018, our most advanced candidate that represents a non-antibiotic, non-steroidal, non-immunomodulatory approach for the treatment of GI disorders including Crohn’s disease,” Enterome CEO Pierre Belichard said in a statement. “We believe we have a world-class partner in Takeda to deliver the best development and commercialization strategy for EB8018 based on their extensive expertise and focus in Crohn’s disease and GI disorders.”
...
Takeda has agreed to pay Enterome $50 million upfront, and a future unspecified equity investment in the company. Takeda has also agreed to pay Enterome up to $640 million tied to achieving clinical development, regulatory, and commercial milestones with EB8018.
Enterome and Takeda agreed to co-develop EB8018, and if approved, co-promote the treatment in the U.S. under a profit/cost-sharing structure. Takeda will receive an exclusive license to commercialize EB8018 outside the U.S., with Enterome eligible for royalties on net sales generated there.
 www.genengnews.com
www.genengnews.com
Takeda has paid $50 million (€44 million) upfront to co-develop Enterome’s early-phase Crohn’s disease candidate EB8018. The deal gives Takeda a stake in a small molecule designed to disarm virulent bacteria and thereby treat gastrointestinal disorders.
EB8018 blocks the activity of FimH, a lectin expressed by enterobacteriaceae such as Escherichia coli. Research suggests the lectin activates TLR4 and thereby encourages the production of TNF-alpha, a cytokine that is the target of Crohn’s drugs such as Humira and Remicade. Enterome hopes EB8018 will prevent production of the cytokine by blocking the local inflammatory cascade.
Backed by preclinical evidence to justify those hopes, Enterome has landed a deal with Takeda. The French biotech will co-develop EB8018 with Takeda and, if approved, co-promote it in the U.S. That ongoing involvement in EB8018 was part of the attraction for Enterome.

Every type of infectious disease has multiple offending agents. In the majority of patients you can identify a specific well defined pathogen, but in around 10%-20%, there are other pathogens involved.It could be highly likely its a combo of pathogens. Malessesiza, AIEC, Map, etc which probably makes more sense, because crohns from patient to patient seems to have a lot of variablity. !
I don't think either doctors or researchers appreciate the fact that almost no one had intestinal issues prior to their disease.I never had a single symptom in my life for 40+ years
For what it's worth, my son had intestinal issues from birth, so I'm pretty sure there's a connection to the later Crohn’s, which seemed to come on gradually. Of course, most people's experience may be completely different.I don't think either doctors or researchers appreciate the fact that almost no one had intestinal issues prior to their disease.
I also don't think that people who don't have crohn's disease realise that the road to crohn's disease was not gradual, it was acute and happened in a matter of days.
What do you mean by these, specifically? I know only Natalizumab, which was notorious for its increasing the risk of JC virus infections. Do you know of any other in this class that is in development, promising, and safer for Crohn’s disease?anti-adhesion molecules
Entyvio (vedolizumab) is also an anti-adhesion molecule (integrin) antibody. It's is approved for Crohn's disease, although some regard it as primarily a UC or Crohn's colititis medication, since it works better in the colon rather than the small bowel. Entyvio also has a pretty good safety profile.What do you mean by these, specifically? I know only Natalizumab, which was notorious for its increasing the risk of JC virus infections. Do you know of any other in this class that is in development, promising, and safer for Crohn’s disease?
Urinary tract infections and Crohn's disease both feature adhesive forms of E coli that stick to the host's cells. You can isolate adhesive E Coli in the urine of people with UTI, you can isolate adhesive E Coli in the stool of people with Crohn's.What do you mean by these, specifically? I know only Natalizumab, which was notorious for its increasing the risk of JC virus infections. Do you know of any other in this class that is in development, promising, and safer for Crohn’s disease?

How common is the AIEC bacteria in the wild though? Is everyone being exposed all the time to this stuff, but it's only causing problems in Crohn’s patients? Or is it something rarely encountered that can induce Crohn’s in healthy people if they get exposed?And just to be clear, bacteria adhering to enterocytes is pathogenic behavior, no bacteria are supposed to be there. Commensal E Coli do not do this, AIEC are 100% pathogenic species. They're not pathobionts, they're pathogens.
This is an infection, a majority of people with ileal crohn's disease are infected with AIEC. We can now consistently confirm this.
Well, remember that AIEC has no easily identifiable genetic marker, if it did tests would not be so time consuming and it would be much easier to test. There is a lot of genetic overlap between AIEC and commensal E Coli.How common is the AIEC bacteria in the wild though? Is everyone being exposed all the time to this stuff, but it's only causing problems in Crohn’s patients? Or is it something rarely encountered that can induce Crohn’s in healthy people if they get exposed?
So the differentiation between non-pathogenic E Coli species and AIEC is made ex post facto, by looking at the behavioural patterns of the bacteria in the presence of the host’s cells?Well, remember that AIEC has no easily identifiable genetic marker, if it did tests would not be so time consuming and it would be much easier to test. There is a lot of genetic overlap between AIEC and commensal E Coli.
But where commensales and non-pathogenic E Coli species won't cause issues, AIEC found in crohn's disease on the other hand, are extremely adhesive and invasive, they are pathogens, they manage to attach themselves to the intestinal wall, they penetrate peyer's patches and invade macrophages.
This is an infection, a majority of people with ileal crohn's disease are infected with AIEC. We can now consistently confirm this.
but we consistently find AIEC sticking to the intestinal lining of crohn's disease patients, all over the world.
We see antibodies related to them, we can now predict who will develop crohn's disease by looking for them, and we see disease that looks like crohn's disease in animals that harbour them.
Well, remember that AIEC has no easily identifiable genetic marker, if it did tests would not be so time consuming and it would be much easier to test. There is a lot of genetic overlap between AIEC and commensal E Coli.
But where commensales and non-pathogenic E Coli species won't cause issues, AIEC found in crohn's disease on the other hand, are extremely adhesive and invasive, they are pathogens, they manage to attach themselves to the intestinal wall, they penetrate peyer's patches and invade macrophages.
The presence of the anti-ompc antibodies does not indicate an infection, it doesn’t even indicate the presence of live E Coli (let alone the AIEC) within the organism, it just means the host immune system encountered at least fragments of E. Coli outer membrane protein at some point. Any claim besides this based on the anti-ompc would be further from what the antibodes indicate, and would be better considered as speculation.we use anti-OmpC to actually diagnose the disease.
Well, if you want more info, I have made a whole topic with every relevant link about AIEC.Could you also cite some of the key studies....
Could you cite some of the key studies...
No, you identify them through PCR tests (to identify virulence genes), antibiotic resistance tests, and through phenotypic traits.So the differentiation between non-pathogenic E Coli species and AIEC is made ex post facto, by looking at the behavioural patterns of the bacteria in the presence of the host’s cells?
We find E Coli specific anti-flagellin / CEACAM6 in CD patients. It's pathogenic E Coli, read the studies in the Index I linked you.it doesn’t even indicate the presence of live E Coli (let alone the AIEC) .

So, providing evidence for your claims is “not worth your time”?Not going to argue about this, not worth my time, be thankful we actually have these tests available to us instead.

I have ileal crohn's, never tried D Mannose.Kiny, you have Crohns right? have you ever tried D Mannose?
I agree, that’s why I asked for citations. Providing evidence for your claims is fundamental for making discussions and inquiries meaningful.I appreciate all insights on this topic, as there is no cure the cause is not known. thus everything is conjecture at this point. I view these discussions as academic and I don't think this is a place to argue, but learn.
That's great, but I suggest you talk about me in another thread and stick to the topic in this one.will make him deserving of looked down upon
I don't necessarily 100% agree with you. This is a message board and not a peer reviewed journal article. When someone posts something it is not necessarily required that they post every source. I have read many of Kiny's posts, and Kiny has posted plenty of sources in the past that I don't think it is necessarily required that Kiny post a source with every assertion.I agree, that’s why I asked for citations. Providing evidence for your claims is fundamental for making discussions and inquiries meaningful.
A person can make whatever claims he wants in his own blog, when he is “writing for himself”; but when communicating in a forum, i.e. within a community, he should base his claims on evidence if he wants to be taken seriously. It’s first out of self-respect, and respect for the community he is writing in that he does this; insisting on doing the contrary will make him deserving of looked down upon.
Right. Altought just like Segal, I believe there was an event between step 1 and 2. Onset of crohn's disease is a rather acute event that looks like a gastrointestinal infection. Foodborne infections in the Western world have become very common and could easily explain the gastrointestinal infiction.Kiny, is your theory basically:
1. Some people have an innate deficiency related to their macrophages, which allows
2. Persistent infection with AIEC, which results in
3. Persistent inflammation, which can be stopped by killing the AIEC
When I mention NOD2 and ATG16L1, I am mostly talking from the perspective of ileal disease. They are important in differentiating ileal from colonic due to the presence of paneth cells in the ileum that don't exist in the colon. Anomalies in NOD2 are primarily relevant to ileal disease.This is all plausible to me, but I question whether #1 has actually been well established. I think something else could take the place of #1 which causes some people to be susceptible to this problem.
I would hope not, it's not the case for UTI, it's a few weeks treatment for UTI.So are fimH blockers another treatment you would have to take forever?

What it has done, is give some researchers millions in research funds, blaming every disease on the microbiome, without ever having to come up with a single proof that the microbiome was actually responsible for it, nor having provided a single practical solution.There is no such thing as a 'healthy microbiome'
Okay, so AIEC infect the macrophage, which in response start producing inflammatory cytokines (like IL-23) to harbour the infection. How come IL-23 antagonist treatment is helping crohn's instead of making it worse.If crohn's disease was simply caused by dysbiosis and the inflammation was a reaction to the dysbiosis, fecal transplants would simply cure the disease. Of course it doesn't, it tends to worsen the disease due to the simple fact you are increasing bacterial load.
In people with crohn's disease in remission, the dysbiosis simply disappears, but of course they are not cured at that point. The dysbiosis is simply a reaction to the inflammatory condition, you see dysbiosis in pretty much every intestinal disease that features inflammation, none of them are actually caused by the dysbiosis, neither is crohn's disease.
To explain the deep transmural tissue inflammation you need to find an intracellular pathogen capable of crossing over from the lumen to the deeper lamina propria where it will activate a macrophage response. AIEC is able to do this, so are a few other pathogens, but the amount of pathogens that can do this is rather limited.
Macrophages and neutrophils take up microbes through phagocytosis, they get killed in the phagolysosome through acidic PH and antimicrobial enzymes.Okay, so AIEC infect the macrophage, which in response start producing inflammatory cytokines (like IL-23) to harbour the infection.

FimH blocker that targets AIEC enters phase 2.
Some researchers call them FimH antagonists, some call them fimbriae antagonists, antibiotics compounds, etc... I prefer FimH blockers, it's easiest to write and remember.
I haven't seen any details, but my guess would be they are D-mannose derived.
To understand these FimH blockers, you kind of need to understand the role of fimbriae. They're a feature of mostly gram negative bacteria, especially pathogenic forms of Enterobacteriaceae. The fimbriae of bacteria kinda look like tentacles that stick out, they are used to adhere to cells (they are not the same thing as flagella, flagella also look like tentacles, but they are purely there for locomotion).
What AIEC basically does in crohn's disease patients, is use those fimbriae to interact with M cells. M cells are like little domes, they are not covered with mucus and they are part of the peyer's patches.
I explained what peyer's patches do extensively in other posts, but all you need to really know to understand a FimH blocker, is that AIEC is exploiting M cells to enter tissue and a FimH blocker will try to stop AIEC from adhering to tissue.
If you can prevent AIEC from entering tissue by interferring with its adherence mechanics, that would be a really good thing since you can halt inflammation at that point and disarm AIEC. Killing it would be even better, but disarming it is the next best thing.
"https://finance.yahoo.com/news/enterome-announces-first-patient-dosed-070000908.html
Enterome announces first patient dosed in Phase 2a trial of sibofimloc in Crohn's disease
Wed, September 23, 2020
Sibofimloc (EB8018/TAK-018) is a first-in-class, orally administered, gut-restricted small molecule designed to reduce inflammation underlying Crohn's disease
Sibofimloc binds FimH, a novel microbiome-derived therapeutic target validated by Enterome, to selectively disarm virulent bacteria in the gut that can cause inflammation without disrupting the local microbiome
PARIS and BOSTON, Sept. 23, 2020 /PRNewswire/ -- ENTEROME SA, a clinical-stage biopharmaceutical company leveraging its unique knowledge of the microbiome-immunoinflammation axis to develop next-generation therapeutics, today announced that the first patient has been dosed in a Phase 2a clinical trial of sibofimloc (EB8018/TAK-018) in patients with Crohn's disease. Sibofimloc is advancing through clinical development under a 2018 global licensing, co-development and co-commercialization partnership with Takeda Pharmaceutical Company Limited ("Takeda"). "
Kiny, a few months ago, Takeda grounded Crohn's prospect Sibofimloc/Eb8018,an FimH blocker, which was previously set for a phase 2 trial before it was terminated because of a lack of enrollees. But,from the results of Fecal Calprotectin, it's not hopeful. How do you think of the results? Is the theory of AIEC also hopeful?FimH blocker that targets AIEC enters phase 2.
Some researchers call them FimH antagonists, some call them fimbriae antagonists, antibiotics compounds, etc... I prefer FimH blockers, it's easiest to write and remember.
I haven't seen any details, but my guess would be they are D-mannose derived.
To understand these FimH blockers, you kind of need to understand the role of fimbriae. They're a feature of mostly gram negative bacteria, especially pathogenic forms of Enterobacteriaceae. The fimbriae of bacteria kinda look like tentacles that stick out, they are used to adhere to cells (they are not the same thing as flagella, flagella also look like tentacles, but they are purely there for locomotion).
What AIEC basically does in crohn's disease patients, is use those fimbriae to interact with M cells. M cells are like little domes, they are not covered with mucus and they are part of the peyer's patches.
I explained what peyer's patches do extensively in other posts, but all you need to really know to understand a FimH blocker, is that AIEC is exploiting M cells to enter tissue and a FimH blocker will try to stop AIEC from adhering to tissue.
If you can prevent AIEC from entering tissue by interferring with its adherence mechanics, that would be a really good thing since you can halt inflammation at that point and disarm AIEC. Killing it would be even better, but disarming it is the next best thing.
"https://finance.yahoo.com/news/enterome-announces-first-patient-dosed-070000908.html
Enterome announces first patient dosed in Phase 2a trial of sibofimloc in Crohn's disease
Wed, September 23, 2020
Sibofimloc (EB8018/TAK-018) is a first-in-class, orally administered, gut-restricted small molecule designed to reduce inflammation underlying Crohn's disease
Sibofimloc binds FimH, a novel microbiome-derived therapeutic target validated by Enterome, to selectively disarm virulent bacteria in the gut that can cause inflammation without disrupting the local microbiome
PARIS and BOSTON, Sept. 23, 2020 /PRNewswire/ -- ENTEROME SA, a clinical-stage biopharmaceutical company leveraging its unique knowledge of the microbiome-immunoinflammation axis to develop next-generation therapeutics, today announced that the first patient has been dosed in a Phase 2a clinical trial of sibofimloc (EB8018/TAK-018) in patients with Crohn's disease. Sibofimloc is advancing through clinical development under a 2018 global licensing, co-development and co-commercialization partnership with Takeda Pharmaceutical Company Limited ("Takeda"). "
 classic.clinicaltrials.gov
classic.clinicaltrials.gov
I tend to agree with you on this, but, I think microbiome does have some sort of role. I am thinking, what if CDED and SCD (both of them containing plenty of fiber, in fact SCD is even called the "banana diet") tend to work so well? What if its not just the EEN way of starving a bad pathogen could work, but also, some specific dietary patterns could help some of our non-pathogenic bacteria flourish enough, so that the pathogenic one gets pushed back and have a very small presence? This would, in my head, explain why so many of us react to foods so differently in the diet - we all have to find a very particular mix of things that create the right conditions for our specific set of microbiome to "bloom", and thats why it can feel so fleeting - because the smallest things can push it out of balance. For example I had a 120 calpro, total clinical remission, eating the same exact foods at the same exact times every day, and then a steak that wasn't cooked well enough practically put me into a (hopefully) small flare 1.5 weeks ago.The involvement of enteric pathogens (bacteria and fungi) in gastroenteritis is well known. E coli, Campylobacter, Staph infections, Salmonella, M tuberculosis, Listeria, Yersinia, B Cereus, opportunistic Candida.
But there has never been a disease where a loss of tolerance towards the microbiota has occured, neither in humans nor animals. The mucosal immune sytem has so many safeguards in place to make sure that can't happen. If anything, you would expect people with crohn's disease to have increased tolerance due to anomalies in NOD2 pattern recognition.
It's possible that changes in the microbiota allow for easier colonisation of pathogenic species.
But I can't support theories that suggest the microbiota is directly involved in the inflammatory cascade, suggesting the inflammation is directed at the microbiome. No disease has ever worked like that, and if it that was the case, you would have inflammation all over the organ which is not the case in crohn's disease.
What if its not just the EEN way of starving a bad pathogen could work, but also, some specific dietary patterns could help some of our non-pathogenic bacteria flourish enough, so that the pathogenic one gets pushed back and have a very small presence?
There's no evidence the inflammation in crohn's disease is targeted at the microbiome.What goes against my theory though is the seemingly complete lack of effectiveness of probiotics in Crohn's disease. But I think probiotics have a doubtful clinical significance at best - perhaps they are just not very good at altering the microbiome in general, or not very good at altering them in the ileum, or they dont have the right mix of bacteria to push out the pathogenic one.