For example, with regard to the features listed as distinct to Crohn's above, I've heard that EEN is less effective for isolated colonic Crohn's - has anyone else heard that?
EN is only slightly less effective in Crohn's disease involving the colon than ileal, we've known this for decades. But the differences are small. The higher up the GI tract you go, the more effective EN seems to be. EN is also effective in treating SIBO.
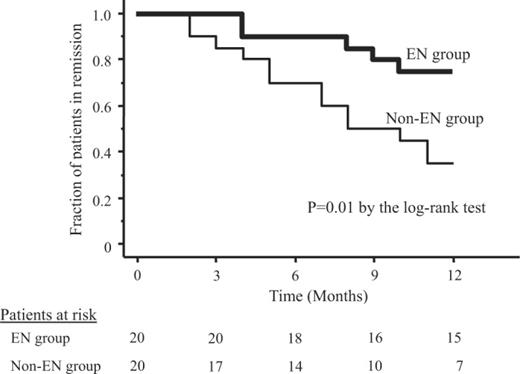
People with ileal disease also remain in remission slightly longer after EN treatment than those with colonic disease. But the differences are always very small.
EN still has much higher remission rates, even in colonic disease, than any other treatment.
https://gut.bmj.com/content/gutjnl/31/10/1133.full.pdf

It prefer looking at older studies. It is hard to take many current studies at face value anymore. Some GI now call IBD "a spectrum" and argue that there are some patients where they can't figure out if they have UC or Crohn's. If you can't figure it out, find a different profession, because it obfuscates treatment for patients. These GI try everything they have in their medicine cabinet until something works, that's not how treatment is supposed to work, treatment needs to be personalized because a large and increasing number of treatments that work for UC do not work for Crohn's disease at all.
This also impacts studies, there have been many clinical trials for crohn's disease that had to be stopped lately, because researchers want specific candidates that meet certain criteria regarding disease location and clinical presence of the disease and the process of diagonsis is not rigorous enough. If you start calling IBD "a spectrum" these researches can't find the right patients. The pathology and medical treatment falls apart, the link between research and medicine becomes clouded and you get contradicting studies.
There was this recent study called "We can't find patients", where researchers lament the fact they can't find the right patients for crohn's disease trials anymore because many patients with colonic disease might not have crohn's disease because of diagnostic failures.
Every anti-inflammatory that doesn't target main cytokine involved in the inflammatory process like TNF and IL23 has failed in crohn's disease. JAK, α4β7, etc, they have all failed to reach high enough remission rates, but they work for UC. UC has a whole laundry list of anti-inflammatories and biologics that work, crohn's disease has very few.
We have clearly reached a plateau on biologics for crohn's disease, where for decades no biologics has improved upon the remission rates of TNF-a blockers, which have existed for decades. Remission rates on biologics are still extremely low and relapse and loss of effectiveness is incredibly common. The only exception has been EN, which has incredibly high remission rates of 88%+.


 62.1 KB Views: 5
62.1 KB Views: 5

")