Hi folks, I posted on this lovely forum at the end of June see below.....Hi all,
Firstly I am not diagnosed but really wanted some insight into the possibility of IBD after a recent upper endoscopy. My GP had arranged this procedure due to my problems with long standing acid reflux and upper abdominal fullness and pain.
Although this was the reason for my endoscopy yesterday I have had years of intermittent and unpredictable diarrhoea and tummy cramps. This had been put down to IBS after an upper and lower endoscopy 4 years ago showed nothing.
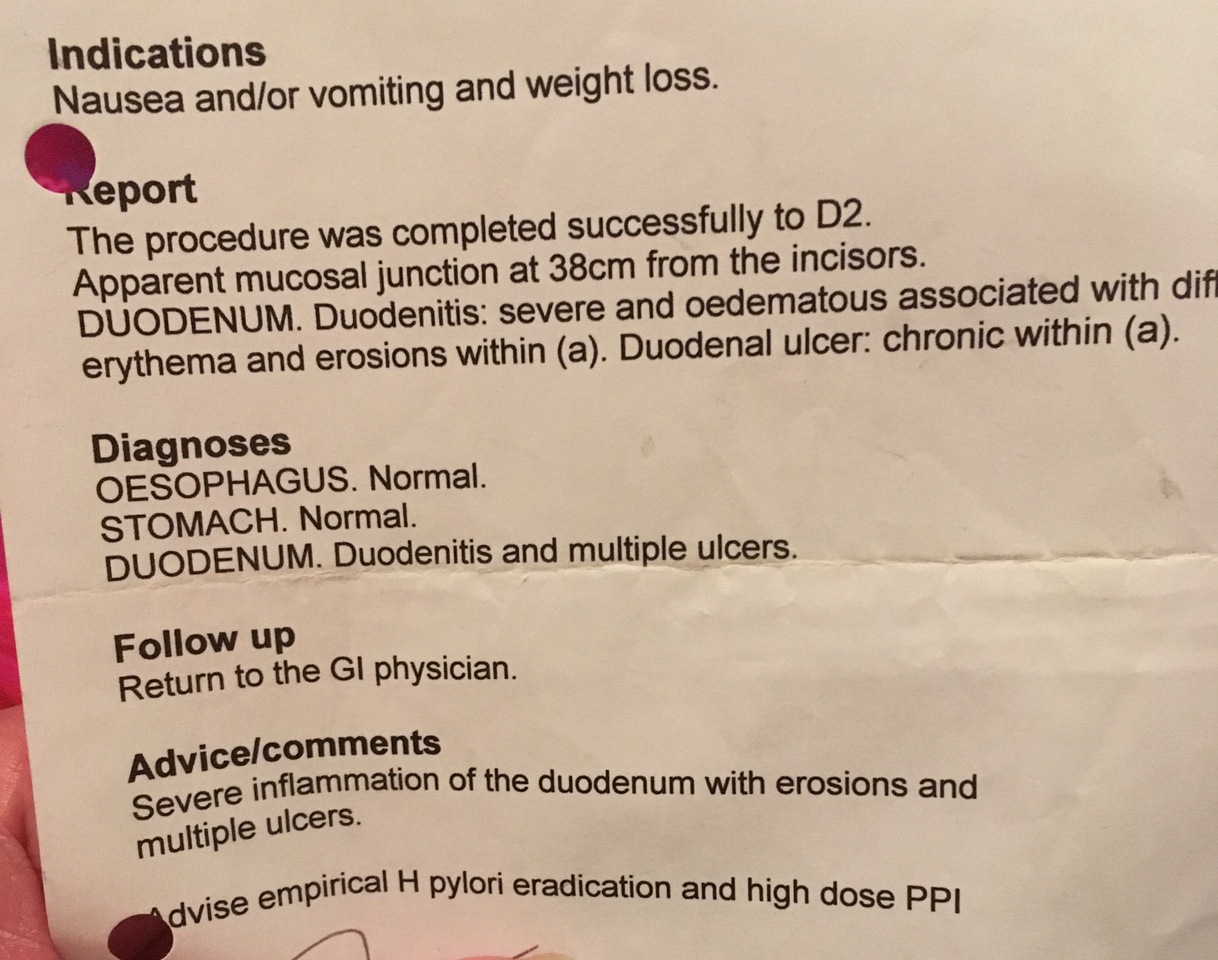
So the GI consultant saw me after the procedure yesterday and told me my gullet seemed fine but he was surprised to see some apthous ulcers in my duodenum. In his report he wrote 'ulcerated localised mucosa' and 'erosions x3 apthous type'
He had done an H pilori test which was negative and previously been negative. He asked me if I used anti-inflammatories much (I don't) as apparently this is the other main cause of erosive duodenitus.
He has taken biopsies and talked of doing a colonoscopy and a scan ??? To check for more of these ulcers. In the procedure comments he has written possible IBD awaiting pathology.
could I please have some thoughts on this ? Are these findings really suggestive of IBD ? And what would the pathologist be looking for in the biopsies ?
Many thanks in advance folks. X
....... I have now received my biopsy results and would love someone to tell me what the results are likely to suggest before my Gi appointment in a couple of weeks....
'Clinical details, heartburn/reflux, duodenal apthous, ulceration ?, crohns.
Biopsy shows 2 fragments of small bowel mucosa, towards the edge of one fragment there is surface ulceration, fibrinous excudate and secondary epithelial regenerative changes. There is no evidence of malignancy. No organisms are identified. Granulomata are not present. The features are regarded as non specific active inflammation and ulceration.'
Firstly I am not diagnosed but really wanted some insight into the possibility of IBD after a recent upper endoscopy. My GP had arranged this procedure due to my problems with long standing acid reflux and upper abdominal fullness and pain.
Although this was the reason for my endoscopy yesterday I have had years of intermittent and unpredictable diarrhoea and tummy cramps. This had been put down to IBS after an upper and lower endoscopy 4 years ago showed nothing.
So the GI consultant saw me after the procedure yesterday and told me my gullet seemed fine but he was surprised to see some apthous ulcers in my duodenum. In his report he wrote 'ulcerated localised mucosa' and 'erosions x3 apthous type'
He had done an H pilori test which was negative and previously been negative. He asked me if I used anti-inflammatories much (I don't) as apparently this is the other main cause of erosive duodenitus.
He has taken biopsies and talked of doing a colonoscopy and a scan ??? To check for more of these ulcers. In the procedure comments he has written possible IBD awaiting pathology.
could I please have some thoughts on this ? Are these findings really suggestive of IBD ? And what would the pathologist be looking for in the biopsies ?
Many thanks in advance folks. X
....... I have now received my biopsy results and would love someone to tell me what the results are likely to suggest before my Gi appointment in a couple of weeks....
'Clinical details, heartburn/reflux, duodenal apthous, ulceration ?, crohns.
Biopsy shows 2 fragments of small bowel mucosa, towards the edge of one fragment there is surface ulceration, fibrinous excudate and secondary epithelial regenerative changes. There is no evidence of malignancy. No organisms are identified. Granulomata are not present. The features are regarded as non specific active inflammation and ulceration.'
")
 )
)